#Surgeon Control Panel
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Premium Tumblr themes are available from anywhere between $9 to $49.
Text

I still have tons to say about the Garashir Goes Canon™ moment in Lower Decks so here is my big meta post about it! Below the cut is a meta discussion about the penultimate Lower Decks episode, contextualizing what it means for something to become canon.
To be clear, this is a mostly positive post with analysis included. You’ll see lots of love for Garashir and Lower Decks and also oodles of fandom meta below the cut, since we have a complicated relationship with Paramount. My analysis and graphic is based on a recent lecture about Star Trek canon I gave at KiScon!
First, I have to say that both Unification and this Lower Decks episode following mere weeks after of my lecture panel at KiScon titled Fuck Paramount, about what Star Trek canon really is and what its place is in relation to us as slash fans, is absolutely mind-blowing timing. I wish everyone in both the K/S and Garashir fandoms had been able to attend it because it was absolutely designed to serve as a framework for both of these major fandom moments. And also it was just funny as hell. But most importantly, it was relevant, and existed to give us a sense of understanding when navigating Paramount hell, particularly when they play Gay Chicken (will they, won’t they — most of the time, they won’t).
Since not every single Star Trek fan on this website was at KiScon last month, I want to expand on that a little more here, this time in Garashir context, since last time it was centered on K/S, though Garashir came up several times! When I was giving my lecture, I asked the audience what it would look like if K/S were made canon tomorrow. Everyone had different ideas—but the most common theme that came up was sheer distrust of Paramount doing it justice.
For those of you that are reading this, the thesis of Fuck Paramount was that you as a fan and a viewer have more control over what is and isn’t canon than you think, and that our role as fans is to take ownership of our stories back from corporate interests. I also developed a four-sided framework to describe how we interact with canon to take power back and make sense of canon. Both Unification and the very, very fresh Lower Decks episode have already been controversial for a number of reasons, the primary one they share being: “Wait… does this make this canon?”
So far it looks like the main reactions for this Lower Decks episode (especially considering how sudden and late in its run it is) are mostly “HOLY SHIT THEY REALLY DID IT” and “I AM DISAPPOINTED BY THE MERE SCRAPS.”
And my position on it is that both of them are completely reasonable reactions that don’t contradict one another! I’m going to make the case for both sides as I try to explore the implications of this episode with respect to the episode’s subtext, corporate storytelling, and so forth. I’m not going to go too much into the academic aspects, but I am happy to make the original slides available for anyone who is curious about my canon analysis framework.
Why It’s Enough
On one hand, this episode is done well. Undeniably. It’s a lot of fun. I have also said many times before that the only way I’d want K/S or G/B to become canon is if they suddenly randomly drop the info that they were married and don’t bring it up again, because otherwise they might do more harm than good! This was an example of it done incredibly well, in my opinion.
This episode serves as all the confirmation you could possibly really need of Garashir. Yes, there are quite a few gimmicks involved—it’s all AU, all the way. Garak is now a surgeon from another dimension, and Bashir is from an entirely different dimension, and also not really himself, but a hologram. Here’s how they’re introduced:
WILLIAM BOIMLER: “Elim Garak, a brilliant Cardassian Surgeon—and his husband, an emergency medical hologram based on Dr. Julian Bashir.”
What I really love about this moment is that it actually does more than it looks like it does, at face value. For most of us, our first instinct is to go, whatever, he’s based on Bashir, he’s not even the real one! But what they did here was brilliant—it serves as implicit confirmation that our man Bashir is also bisexual, and loves Garak. He is indeed not a corporeal human being, but as the DS9 episode where the LMH is designed based on Bashir tells us, the hologram is designed and based on who he is. It has his personality traits. Interviews are conducted to make sure that the hologram is as authentic and true to the real thing as possible:
O'BRIEN: “You mean this programme is going to have all of his personal likes and dislikes?” ZIMMERMAN: “That is why we bother to choose a human template in the first place.”
William Boimler, from the prime Star Trek universe, doesn’t say the EMH is based on some Bashir, he says this one is based on Dr. Julian Bashir. Again, this serves as clear confirmation that he is modeled on recognizably the same character from DS9. They’re not that different in essence from their prime universe counterparts, or it wouldn’t be fun for the writers or the audience. We learn that Garak is still former Obsidian Order. They are still the same people, in essence. They may be AU characters but the point is for them to be similar to the originals, or they may as well just have been some guys!
The important thing, for me, is that it’s a clear, unambiguous acknowledgement. It’s played straight. Well, not straight—but not as some elaborate joke or filled with contempt. It doesn’t tease and doesn’t dance around the issue and wink and nudge, begging the viewer to question whether or not they’re together. That much is made immediately very clear. In the episode, AU Garak and AU EMH Bashir are a married couple, and they kiss. Every moment of their relationship is sincere, the comedic moments being not about the fact that their relationship exists, but about the dynamics it brings to the story. It also tells us very clearly that they’re not even from the same universe, and that their compatibility remains nonetheless:
HARRY KIM: “Are they from the same reality?” CURZON: “No, but they love to brag about how statistically unlikely their marriage is.”
Again, I tend to see this as a positive nod to the compatibility of these characters rather than a brush-off that says the prime universe Garashir couldn’t be together. And then Garak tells us his universe’s Bashir is like the original: still a racquetball player and competes with Chief O’Brien—again, revealing quite a bit.
And the B-plot is about them squabbling, acknowledging very clearly to us that Cardassians really do just love flirting via argument, which serves as a brilliant nod to everyone who complained for three decades that the DS9 writers never really admitted that Bashir and Garak were just flirting. Finally! The writers seem to understand quite well what’s important to us, even if this isn’t the ‘Real Garashir.’
What satisfies me ultimately is that this doesn’t in any way look like a rejection of the possibility of Garashir in the prime universe. It looks to me like it supports the text, not a mean-spirited denial that it could only happen under bizarre AU circumstances. To sum it up with another Boimler quote:
BOIMLER: “The multiverse is just a rehash of stuff I already know.”
Hm… :)
And as I pointed out in a prior post, the whole point of the episode is to show that even in different circumstances and worlds, the love characters have for one another remains a constant and is utterly transcendent. The episode straight up tells us that some relationships are so powerful that they span dimensions and realities, and then Garak and Bashir say they would follow one another to any reality!
In my panel-lecture, I said, “[Paramount’s control over the text] suggests that certain readings require their endorsement or confirmation to be true.” But this doesn’t feel like that to me, and so I accept this. It leaves room for possibilities of all kinds, and opens more doors rather than closing them. I can appreciate that.
I also spoke about how canon isn’t one thing—not a binary yes or a no, and that there is no singular meaning. I call this multiplicity:
“Multiplicity is about the continuous proliferation of ideas and the rejection of the text as having a single meaning. It rejects mere viewing or the consumption of media in favor of dialogue and participation rather than a one-way communication.”
This episode served to defy singular interpretations of the text. It tells us that there are infinite possibilities and it took a route that challenges the single-story interpretation of Garashir = Not Canon. It made room for new perspectives and affirmed what “the stuff we already know.”
Why It’s Not Enough
Now for the other side of the coin: why it’s not enough. As exciting as it is to have this kind of confirmation from the current writers for Star Trek in a frankly increasingly conservative storytelling environment, it’s still disappointing for many people that even in the most progressive Star Trek that exists, they cannot or will not openly state that the prime universe Garashir got the ending and acknowledgment they deserved.
It feels like begging Paramount as a corporation for scraps and thanking them for what really doesn’t feel like enough—it stops short of full, sincere, complete validation of Garashir’s queerness. As I said in my panel, it’s normal for us to want confirmation from the writers and creators that what we’re seeing is real and not just imagined, even when the role of fanfiction is for us to transform canon and reject it ourselves.
It’s absolutely exhausting for us to say we see something that is continuously denied by those who ‘own’ the story in favor of mass appeal, and to me, that is a legitimate perspective that can coexist with the idea that fandom is designed reshape the canon to fits its own needs, and that we don’t need confirmation from the creators for something to be true. Fandom exists to defy corporate ownership of stories, but to have to fight for mere moments where marginalized perspectives are foregrounded causes anger for good reason. We may not need confirmation from them, but saying that we should never expect anything from Paramount releases the corporation of accountability and obligation to respect the audience and their own characters. We should be able to expect and trust that these characters and their relationships can be done justice by those who have the privilege of steering that ship.
It’s one thing for me to say that this episode affirms the reality of Garashir, but it’s also true that prime Garashir probably could not be given complete canonization because this is the best way they knew how to ‘get away with it’ all while maintaining its mainstream and popular appeal with heteronormative audiences that would have a problem or reject it if it happened to ‘real Garashir.’
Slash fans, for decades, have existed in the lane of compromise—firmly between having our truth validated and entirely rejected in favor of a Star Trek that is designed to be sold as a product to as many people as possible. Rarely do we receive more than a bone tossed to us by the powers that be, and when we do receive it, it’s on their incomplete terms, often with massive concessions made to make it happen. For Garashir to receive their blessing, they had to twist it into an AU. The reason they could do this episode is because it gave them the neat plausible deniability to also say this has nothing at all to do with prime Garashir, so that it didn’t entirely alienate audiences who wouldn’t support a queer narrative.
This is their way of having their cake and eating it too. In some ways, it looks like they’re just trying to make everyone happy, but the story shouldn’t have to make everyone happy, and a compromise can really just feel like everyone loses, or like prioritizing the status quo again. For decades, the status quo has always left those with marginalized readings of the text unhappy, sidelined by a narrative that is supposed to be progressive and supposed to look to a future where queerness is natural and not taboo. And if this is the best they can do, it’s only reasonable that it should still sadden us, disappoint us, anger us. It’s hard not to resent that reality.
What Now?
I urge folks to continue negotiating the text, as I did above in the first section. I made sense of it in a way that fits my understanding of Garashir! You do not have to assume that there’s no more to it than that because it was all that was said on screen. We don’t have to look at canonization as the final say on the text. My perspective is that we should take it as a wonderful and deserved affirmation, and continue to transform the canon as we see fit. This is your time to decide what it means for these characters. Personally, I see it as a massively positive step forward. Just remember that where canon is concerned, you are in control of what it means.
Canon is still transformable, multiplicative, negotiated, and timely. Holders of the ‘IP’ are only one piece of the puzzle where the truth of a story is concerned. So take this as a beginning to more, not an end! As I like to say, “canon is a means to an end, not the end itself.”
Also, please don’t hesitate to add your thoughts, questions, comments, or anything else. I hope you enjoyed this meta post, if you read this far.
#star trek#star trek meta#lower decks#ds9#deep space nine#garashir#elim garak#julian bashir#garak x bashir#I hope you enjoyed this post and found it fascinating!
101 notes
·
View notes
Text
The Best News of Last Week
🦾 - High-Five for Bionic Hand
1. Houston-area school district announces free breakfast and lunch for students

Pasadena ISD students will be getting free breakfast and lunch for the 2023-24 school year, per an announcement on the district's social media pages.
The 2023-24 free lunch program is thanks to a Community Eligibility Provision grant the district applied for last year. The CEP, which is distributed by the Department of Agriculture, is specially geared toward providing free meals for low-income students.
2. Dolphin and her baby rescued after being trapped in pond for 2 years
youtube
A pair of dolphins that spent nearly two years stuck in a Louisiana pond system are back at sea thanks to the help of several agencies and volunteers.
According to the Audubon Nature Institute, wildlife observers believe the mother dolphin and her baby were pushed into the pond system near Grand Isle, Louisiana, during Hurricane Ida in late August 2021.
3. Studies show that putting solar panels over waterways could boost clean energy and conserve water. The first U.S. pilot project is getting underway in California.

Some 8,000 miles of federally owned canals snake across the United States, channeling water to replenish crops, fuel hydropower plants and supply drinking water to rural communities. In the future, these narrow waterways could serve an additional role: as hubs of solar energy generation.
4. Gene therapy eyedrops restored a boy's sight. Similar treatments could help millions

Antonio was born with dystrophic epidermolysis bullosa, a rare genetic condition that causes blisters all over his body and in his eyes. But his skin improved when he joined a clinical trial to test the world’s first topical gene therapy.
The same therapy was applied to his eyes. Antonio, who’s been legally blind for much of his 14 years, can see again.
5. Scientists develop game-changing vaccine against Lyme disease ticks!

A major step in battling Lyme disease and other dangerous tick-borne viruses may have been taken as researchers announced they have developed a vaccine against the ticks themselves.
Rather than combatting the effects of the bacteria or microbe that causes Lyme disease, the vaccine targets the microbiota of the tick, according to a paper published in the journal Microbiota on Monday.
6. HIV Transmission Virtually Eliminated in Inner Sydney, Australia

Sydney may be the first city in the world to end AIDS as a public health threat by 2030. Inner Sydney has reduced new HIV acquisitions by 88%, meaning it may be the first locality in the world to reach the UN target to end AIDS as a public health threat by 2030
7. New bionic hand allows amputees to control each finger with unprecedented accuracy

In a world first, surgeons and engineers have developed a new bionic hand that allows users with arm amputations to effortlessly control each finger as though it was their own body.
Successful testing of the bionic hand has already been conducted on a patient who lost his arm above the elbow.
----
That's it for this week :)
This newsletter will always be free. If you liked this post you can support me with a small kofi donation:
Support this newsletter ❤️
Also don’t forget to reblog.
897 notes
·
View notes
Text

By: Gerald Posner
Published: Mar 4, 2024
Newly leaked files from the world’s leading transgender health-care organization reveal it is pushing hormonal and surgical transitions for minors, including stomach-wrenching experimental procedures designed to create sexless bodies that resemble department-store mannequins.
The World Professional Association for Transgender Health documents demonstrate it’s controlled by gender ideologues who push aside concerns about whether children and adolescents can consent to medical treatments that WPATH members privately acknowledge often have devastating and permanent side effects.
Yet the US government, American doctors and prominent organizations nonetheless rely on WPATH guidelines for advice on treating our youth.
The files — jaw-dropping conversations from a WPATH internal messaging board and a video of an Identity Evolution Workshop panel — were provided to journalist Michael Shellenberger, who shared the documents with me.
Shellenberger’s nonprofit Environmental Progress will release a scathing summary report, comparing the WPATH promotion of “the pseudoscientific surgical destruction of healthy genitals in vulnerable people” to the mid-20th-century use of lobotomies, “the pseudoscientific surgical destruction of healthy brains.”
‘Arbitrary’ age limits
The comparison to one of history’s greatest medical scandals is not hyperbole.
It is particularly true, as the files show repeatedly, when it involves WPATH’s radical approach to minors.
When the organization adopted in 2022 its current Standards of Care — relied on by the National Institutes of Health, the World Health Organization and every major American medical and psychiatric association — it scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries.
It had previously recommended 16 to start hormones and 17 for surgery.
Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones.
During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4.
The child insisted on a vaginoplasty, a surgery that removes the penis, testicles and scrotum and repositions tissue to create a nonfunctioning pseudo-vagina. It requires a lifetime of dilation. Was he too young at 14?
Marci Bowers, WPATH’s president and a California-based pelvic and gynecologic surgeon who is herself transgender, said she considered any age limit “arbitrary.”
But she would not do it. Why?
“The tissue is too immature, dilation routine too critical.”
In lay terms, that means boys who are too young do not have enough penal tissue for the surgery and the surgeon must harvest intestinal lining to build the faux vagina. Even Bowers admits that can lead to “problematic surgical outcomes.”
She would know since she has performed more than 2,000 vaginoplasties. Her highest-profile patient is 17-year-old Jazz Jennings, the transgender star of reality TV show “I Am Jazz.”
Three corrective surgeries were required to fix problems from the original vaginoplasty.
“She had a very difficult surgical course,” Bowers admitted in a 2022 appearance on the show. “We knew it would be tough — it turned out tougher than any of us imagined.”
Still, Bowers told her colleagues in the internal discussion forum of the best age for an adolescent to undergo surgery: “sometime before the end of high school does make some sense in that they are under the watch of parents in the home they grew up in.”
Christine McGinn, a Pennsylvania plastic surgeon and herself transgender, agreed. McGinn has performed “about 20 vaginoplasties in patients under 18” and thinks the “ideal time in the U.S. is surgery the summer before the last year of high school. I have heard many other surgeons echo this.”
Waiting until teens are older than 18 and in college is problematic, she said: “there are too many stressors in college that limit patients’ ability to dilate.”
Dangers downplayed
WPATH assures patients that surgical and hormonal interventions are tested and safe. It is a different matter in private.
President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
What about children who are infertile for life since they started hormone blockers before they reached puberty?
Bowers told her colleagues the “fertility question has no research.”
At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue.
It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused. Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.”
Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”).
Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.”
One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
Rise of ‘de-gender’ surgery
The litany of transition surgery’s side effects did not stop WPATH from endorsing far more radical “nullification” surgeries for patients who do not feel either male or female and identify only as nonbinary.
Several dozen so-called “de-gendering” surgeries are designed to create a sexless, smooth cosmetic appearance that is unknown in nature. There is even an experimental “bi-genital” surgery that attempts to construct a second set of genitals.
In 2017, when tabloids reported a 22-year-old man had spent $50,000 to surgically remove his sex organs so he could “transform into a genderless extra-terrestrial,” it seemed a one-off oddity.
But WPATH has enshrined that concept in its Standard of Care — the same document in which the group endorsed for the time first time chemical or surgical castration for patients who identify as eunuchs. (WPATH even linked to the Eunuch Archives, where men anonymously share castration fetishes.)
These science-fiction-like surgeries are not only reserved for adults.
“How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.”
What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
The goal, as one San Francisco surgical clinic proclaims on its website, “is a smooth, neutral body that is cosmetically free of sexual identification.” On TikTok the trend is called a “flat front.”
‘Too young to understand‘
A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation.
Gender surgeries are an exception, however.
WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible.
Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
Metzger noted adolescents are incapable of appreciating the lifelong consequence of infertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old,” he said, “but I know I’m talking to a blank wall. They’d be like, ‘ew, kids, babies, gross.’ Or, the usual answer is, ‘I’m just going to adopt.’ And then you ask them, ‘Well, what does that involve? Like, how much does it cost?’ ‘Oh, I thought you just like went to the orphanage, and they gave you a baby.’ . . . I think now that I follow a lot of kids into their mid-twenties, I’m always like, ‘Oh, the dog isn’t doing it for you, right?’”
There is extensive research showing adolescent brains are wired to have little control over rash behavior and are not capable of grasping the magnitude of decisions with lifelong consequences. It is why society doesn’t allow teens to get tattoos or buy guns. Car-rental agencies set 25 as the minimum age for renting a car, and Sweden sets the same limit for deciding on sterilization.
Detransitioners ignored, shunned
Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.
Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.
WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.
It’s a question that would never be asked for minors who declared themselves to be gender dysphoric.
One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”
A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
WPATH President Bowers said that “I do see talk of the phenomenon [detransitioners] as distracting from the many challenges we face.”
‘Frankenstein files’
The leaked files put a spotlight on the danger of mixing ideological activism with medicine and science. They should serve as an urgent wakeup call for the medical associations and government agencies that rely on WPATH guidance for transgender health.
The files might even prompt investigations into how those with distorted personal agendas seized control of the organization at the expense of science and patients.
Investigating what has gone wrong at WPATH might prove uncomfortable for some gender progressives in the Biden administration, none more so than Adm. Rachel Levine, the assistant secretary for health. Levine, the first transgender four-star military officer, is a WPATH member and has lavished praise on the organization.
She says it “assesses the full state of the science and provides substantive, rigorously analyzed, peer-reviewed recommendations to the medical community on how best to care for patients who are transgender or gender non-binary. It is free of any agenda other than to ensure that medical decisions are informed by science.”
Either Levine is unaware of the hormonal and surgical experimentation the group promotes or refuses to acknowledge it.
“The Frankenstein files.”
That is how a pediatrician described the leaked documents after I shared them with her.
Unfortunately, this is no horror novel.
It is a medical travesty playing out in real time, and the casualties are our children.
#Gerald Posner#Michael Shellenberger#WPATH#World Professional Association for Transgender Health#Mia Hughes#WPATH Files#The WPATH Files#medical corruption#medical malpractice#medical scandal#unethical#gender ideology#gender identity ideology#queer theory#first do no harm#religion is a mental illness
32 notes
·
View notes
Text
Little Tea Cakes (Jean x Reader)
Synopsis: You and Jean were left to hold down the fort, but when night falls, and your friends aren’t back yet, you start to worry. Jean has the perfect plan to take your mind off of things and enjoy your cozy night in.
Word Count: 2k
Tags/Warnings: Fluff
Notes: I’m ready to make this recipe

You stared out the window, practically curled up on the ledge as you waited. Jean had lit lanterns that flickered on the outside porch. If it weren’t for those, you wouldn’t have been able to see how the rain poured down in sheets outside in the blackness.
You saw his reflection as he loitered behind you, unsure what to say. With the night as dark as it was, you could see in the glass how his mouth opened and closed again as he put his hands on his hips. He stared momentarily, watching as you kept your eye on the night.
“They’re fine,” he finally said. Jean slipped his fingers into the pockets of his slacks. He didn’t exactly sound sure of himself. “I’m sure they’ll be back any minute now.”
“It’s coming down really hard out there,” you trailed off, rubbing the underside of your bottom lip with your finger. A large puddle had begun to form at the bottom of the wooden steps outside your cabin. You looked over your shoulder at Jean. “What if something happened to them, and they need our help?”
Jean came to stand next to you, leaning the slightest bit back against the dining table. He stood with you, looking out the window at the storm. The wind howled outside, causing a few hung lanterns to sway and knock against the wood paneling. You watched the reflection again as Jean bowed his head acutely toward you. You noted the shrug of his shoulders.
“Captain Levi’s with them. They’re probably just caught up kickin’ ass.” Jean gave you a gentle nudge, but you couldn’t tear your eyes away from the window.
A moment went by as the rain continued to pour. You found yourself lost in your worries, hardly registering as Jean pivoted to stand in front of you. A warm touch found your forearm. Your head shot up as you broke out of your daydreaming, and he gestured again with his head.
“C’mon,” he said with a semblance of a sigh. You blinked a few times, caught off guard by your own spacing. Jean tugged at the fabric of your sleeve, gesturing again toward the kitchen. He repeated himself, and reluctantly, you let yourself be dragged over to the sink. You looked back over your shoulder.
“But—”
“They’re fine.” Jean washed his hands with the rigor of a surgeon, leaving the water running as he motioned for you to do the same. You followed as he proceeded to raid the cabinets. You waited, drying your hands on a towel hung on the island in the center of the kitchen.
Jean closed a cabinet somewhere to your left. You almost jumped as Jean placed a large mixing bowl in front of you. You stared into his honey-colored irises.
“No use in worrying about something you can’t control.” He ducked down for a moment to pull something out of the island’s storage. Jean placed the container on the counter and shoved a cup between your fingers. “Two of those in the bowl,” he said, patting the container.
You did as you were told, and by the time you were finished, several other supplies had appeared on the counter. He handed you a series of spoons, giving similar instructions for the next three ingredients before Jean wandered off to start the oven. The rain continued to pour outside.
“What are we making?” you finally asked, staring down at the bowl of mixed powders. Jean appeared to your right with a pile of sliced butter cubes and a tool that looked more like a claw than a kitchen utensil.
“Tea cakes,” he answered softly, dumping the butter into your mixture. He handed you the claw. “My mom used to make them on rainy days. I’m sure everyone will love them when they get back.” You stared at the appliance in your hand, missing the pink that tinged Jean’s cheeks.
“What am I supposed to do with this?”
“It’s to mix the butter in so that the mixture becomes crumbly.”
You gave him an uneasy look, gingerly placing the pastry cutter into the mixture and attempting to mix. Jean hummed apprehensively, his hand hovering over the bowl before firmly placing it over yours.
“Like this,” he muttered, maneuvering himself behind you as he guided your hand. He held your opposite elbow as you kept the bowl steady, almost as if you’d shatter in his arms at any moment. Focused on your task, you hardly noticed the bright shade of red that slowly overtook the pink on Jean’s face.
Once the mixture turned crumbly and the butter was well incorporated, Jean pulled away from you, his retreating body heat leaving a small chill in his wake. He exchanged your larger bowl of dry ingredients for a smaller one, placing two eggs in front of you with a cup of milk, honey, and a tiny dish of flavoring. During the time it took to measure the dry materials, it had apparently been enough time for him to portion out all the wet ingredients.
One by one, you added them to the new bowl. Jean took the discarded eggshells for the compost and tiny dishes that held the preportioned ingredients to the sink. You went to place the pastry cutter back into the bowl of wet ingredients to demonstrate what Jean had just taught you, but Jean gently replaced the claw with a wooden spoon instead.
You smiled at him sheepishly. Jean leaned on the counter, ankles crossed as he leaned on his elbows, watching as you beat the wet ingredients. Once incorporated, you were instructed to pour the liquid into the flour mixture. Jean watched you work as raindrops continued to hit the rooftop.
“See, you’re already getting the hang of it.” Jean nodded. You worked the spoon to incorporate the bit of flour left over on the side of the bowl.
“Did you eat these a lot growing up?” You slide the finished batter toward him. Jean had already prepared a greased baking tin.
“More than I’d like to admit.” He let out a light chuckle. The softness in his voice wasn’t lost on you as he spooned the batter into the tin. He scraped down the sides before handing you the bowl to put in the sink. “A lot of rainy days, I guess.”
You took to the dishes as he placed the tin in the oven. You stared out the window as the remaining batter stuck to the bowl washed down the drain. You were just starting to wonder what you did on rainy days as a kid when you felt a gentle nudge.
“I got it,” Jean said, gradually prodding you out of the way until you had no choice but to leave the bowl and sponge. His sleeves were rolled up to his elbows, and once the sponge had been replenished with soap, he took to vigorous scrubbing.
You studied him: the way his bangs waved with his efforts, the curve of his nose, and the squareness of his chin. He placed the first clean bowl onto the drying rack, eyes flickering up toward the window for a split second as a clap of thunder resounded throughout the sky. Jean pursed his lip, and as he met your gaze briefly, he quickly glanced away. You wondered if he was as secretly worried as you were.
You tugged open the cabinet to your right. Luckily, the kettle didn’t sit too high up.
Jean had just finished the dishes by the time you came to fill up the kettle. His brows twisted up in confusion as you pivoted the faucet. You offered him a shrug. Jean dried his hands on a nearby rag.
“You said tea cakes. What’s a tea cake without tea?”
“Mama always served them with milk,” he trailed off, the movement of his hands slowing as he found himself lost in thought. The realization of what he said aloud must’ve hit him instantly. His eyes widened, only to be met with your mounting expression of amusement. “I, uh—! I mean—”
“Don’t worry, Jean-boy. I’ll grab some milk,” you said, putting the kettle on before making a beeline to the fridge. Jean continued to fidget with the towel in his hands.
“You really remember that?” he asked sheepishly, a twinge of cringe causing his eye to twitch. You prepared two cups, placing a milk carafe between the two of you. The air in the kitchen had already begun to smell sweet.
“Nothing wrong with having a mother who loves you.” You poured him a glass of milk. “How is she doing?” You stood across the island from him, watching the oven.
“She’s alright.” Jean nodded, slowly picking up the cup. He brought it to his lips. “I think she gets anxious while I’m away. Lonely.” You played with your empty cup with a sigh.
“That must be tough… You should visit her when all of this is over. I’m sure that after all the chaos, we’ll get to take a bit of a break.” Jean let out an amused puff, staring off at the near-boiling kettle.
“Think so?”
“I’m sure she’d be happy to see you. Know that you’ve been thinking about her.” Jean didn’t get a chance to respond, cut off by the high-pitched whistling of the tea kettle. You perked up in surprise. “Oh, that was quick.” You grabbed the hand towel that Jean had thrown on the counter.
“I should probably pull out the tea cakes.”
By the time you reconvened at the kitchen island, Jean had already put down two trivets. The tea cake had puffed up into a golden, brown pastry that steamed deliciously in the dark pan. You fixed yourself a cup of tea, cooing over the hot dessert.
“That looks so good!” you exclaimed, the smell alone making you impatient to try. The corners of Jean’s lips twitched upward into a boyish grin. He gestured to you with a bow of his head.
“Well, it was all you. You should be proud of your good work,” he said, leaning the side of his cheek in his palm as he studied the shiny top. “I’ll cut it into squares when it cools down a little.” The thunder that cracked outside sounded so far away.
“Thank you,” you said, playing with the warm rim of your cup. “For distracting me and for sharing this.” You met his eye just in time to see the visible gentleness overtake his expression. Jean’s shoulders relaxed as he nodded.
“Of course.”
A figure moved on the balcony, passing through your peripheral. Just as quickly as you saw it, the front door slammed open. A dripping-wet Captain Levi stormed through the door, removing his boots at the entryway before stalking to his quarters. He gave you a stout, meaningful look as he went, and wordlessly, you worked on preparing him a cup of tea. The rest of the squad followed, a chorus of compliments about the aroma from the kitchen jumbled together as the squad shuffled to the kitchen.
“Oh wow!” Sasha cried, practically drooling at the sight of the warm, golden pastry. Jean shooed her away, waving the hand towel at her as he protected the dessert the two of you had worked so hard on.
“Hey! You’re dripping everywhere!” he chided with a scowl. Jean crossed his arms. “There’s enough for everyone once you’re dry.”
“You don’t gotta tell us twice. I’ve been wanting to change out of these wet clothes all day.” Connie tugged at Sasha’s leather straps in exhaustion. “C’mon, I’m ready to get warm.” You pulled out some more mugs.
“I’ll make everyone some tea!” you smiled, relieved that all your friends made it back safe. You missed the sentimental expression on Jean’s face as he stared at you.
“I’ll cut the cake!”
Thank you to all who liked, reblogged, followed, and supported. Your support means so much and is greatly appreciated.
Notes: I am definitely Jean when it comes to baking, so it was kinda fun writing someone who doesn’t bake haha. It was hard writing this because all I did was want to make the recipe! Maybe one of these days I’ll work in the kitchen to perfect a nice honey tea cake recipe and I’ll post the link here lmao. It’ll be “Kirstein Tea Cakes”!
I feel like the tea cakes were supposed to be made in something like a cupcake tin. But I also thought that Jean’s mom might not have one of those. Or maybe being a mom it’s easier to just put the batter all in one dish, hence why Jean calls them tea cakes when it’s just one cake sliced into squares.
#jean x reader#jean kirschstein x reader#jean kirschtein fluff#jean kirstein#aot x reader#attack on titan x reader#shingeki no kyoujin x reader#shingeki no kyoujin#reader insert#x you#x reader#aot x gn!reader#aot#snk
96 notes
·
View notes
Text
SLEEPBOUND INFO DROP
RAHHHH
as we come close to a month till auditions close, heres some info + doodle sheet

IN DOODLE ORDER (L to R)
VANJA S. The main ‘speaker’ of Sleepbound! They’re a worrywart but never tend to show it. They’re one of the heads of the Astralis and honestly enjoys their job as the Chief Officer.
PRECIOUS ‘MOTHMAN’ Z. Precious isn’t seen too much in the series -albeit being the captain. She’s cold and extremely harsh. Besides that, she means well! At least according to D.E.F.
DELTA ECHO FOXTROT The random space nerd from god knows where. He’s a rather happy and relaxed engineer with an insane love for Star Trek. Although being the resident human, he’s more cyborg like from…. eh who gives a fuck
DAVAA K. The Dragonborn lead surgeon. Unlike what his title suggests, he’s a ball of energy. A very lively and loud man. Even when he tries to help, he’s a little bit of a big mouth. But behind that is some poor overprotective soul just waiting to help.
RAFEN A. The last person on the sheet. He’s a little silly guy, tending to the main control panels with the control team. Not much is known about them besides the fact that they work like an absolute bitch. Maybe you’ll meet them soon! Who knows.
2 notes
·
View notes
Text
Why a High-Quality X-Ray Image Can Make or Break a Diagnosis or Surgery
In modern healthcare, an X-ray image is like a doctor’s second pair of eyes. From diagnosing bone fractures to guiding high-precision spinal surgeries, a clear, properly positioned X-ray image is the cornerstone of accurate clinical decision-making.
So, what makes a truly “high-quality” X-ray? Let’s explore the answer through the lens of Perlove Medical’s professional imaging technology.

1. Proper Patient Positioning = Valuable Imaging
Some patients present previous X-rays that are tilted, misaligned, or poorly centered — making it hard for doctors to accurately assess the problem. Poor positioning can lead to misjudgments or missed diagnoses.
Perlove Medical’s digital radiography systems (such as the PLX5100 and PLX5500) feature precision positioning mechanics and smart interfaces that help radiographers quickly align the imaging region, ensuring scientifically accurate patient posture and image angles — so doctors don’t have to “guess.”
2. Clear Image Quality Builds Clinical Confidence
Image sharpness directly determines whether the doctor can “see” key anatomical structures. Perlove Medical’s high-end dynamic DR and mobile C-arm systems use advanced flat panel detectors and proprietary image processing algorithms to deliver high-resolution, high-contrast, low-noise images. This clarity reveals fine details — from fracture lines to soft tissue contours.
For example, during spinal procedures, surgeons rely on a clear visualization of the “cat’s eye” sign — a critical X-ray landmark that helps ensure screws are precisely placed within the pedicle. Perlove’s mobile C-arm systems (like the PLX118F and PLX7500) are tailored for such demanding tasks, providing high frame rates and instant imaging that enhance intraoperative precision.
📌 Knowledge Tip: The “cat’s eye” refers to the pedicle shadow in anteroposterior (AP) X-ray views, resembling a feline pupil. It’s a key visual indicator for proper pedicle screw placement.
3. Proper Exposure — Not Too Bright, Not Too Blurry
Overexposed or blurry images can obscure diagnostic details. Perlove Medical’s DR systems are equipped with Automatic Exposure Control (AEC) technology, which intelligently adjusts radiation levels based on tissue density — protecting the patient while ensuring image clarity.
Meanwhile, intelligent image optimization enhances contrast and detail across regions of interest, including bone, soft tissue, and metallic implants — making Perlove’s systems ideal for orthopedics, emergency care, neurosurgery, and beyond.
4. 2D + 3D Imaging = Safer, Smarter Surgeries
Traditional 2D X-rays require surgeons to rely on experience to judge depth and alignment — leaving room for error. Perlove Medical’s advanced 3D C-arm (such as the PLX7200) supports real-time 3D reconstruction, upgrading standard fluoroscopy to a 3D view that reveals bone structure and implant paths in detail.
Surgeons can directly visualize whether a screw is safely inside the pedicle or deviated from its intended path — enabling accurate intraoperative adjustments, increasing safety, and boosting the success rate of complex surgeries.
🎯 Conclusion: Clinical excellence begins with clear imaging — and behind every high-quality X-ray is a high-performance device. Perlove Medical is committed to empowering medical professionals with advanced imaging solutions that help them see better, decide faster, and operate with greater precision.
📍 For more product information and clinical case demonstrations, please visit the Perlove Medical official website or contact an authorized distributor.

1 note
·
View note
Text

@climatact - Canon // Dragon Girlfriend - continued from here.
If he was surprised to find the woman here, shoulder-deep in his dresser as she rummaged for a hidden compartment that did not exist, Law gave no indication. If anything, the doctor seemed amused by her antics, a derisive snort filling the space between them as he shook his head at the carefree admission that no, not only had she torn his sock drawer apart - she’d already helped herself to his desk, as well. And no, she was not sorry or embarrassed in the least to be caught in the middle of this invasion of his privacy.
Of course she wasn’t: he’d be in the entirely wrong relationship if he’d expected anything different. If he hadn’t caught the moment of recognition in Nami’s chestnut orbs the second she’d laid eyes on the necklace he’d presented her with just before they’d last parted ways.
With the earrings, although Law hadn’t been there to see the navigator’s initial reaction (thanks in part to his own carelessness and a complete lack of self control/patience on her part), he’d had the sense of quiet surprise - upward turn of her full lips and the occasional glance she’d cast him in passing that evening suggesting she hadn’t expected him to notice her appreciation for that very pair a few weeks prior.
Didn’t she realize he was always paying attention to her? That he knew her too well not to know she’d be a woman on a mission from the moment those precious stones had settled against her collarbone?
No. Law had learned his lesson the first time around. There was a ring, but he wasn’t going to tell Nami that until he was good and ready to slide it onto her finger himself - and he didn’t care how crafty the Thief Cat thought herself: she wasn’t going to find it before then. Lips curled into a self-satisfied smirk as he tilted his head to the side, her withering stare met with an unruffled shrug of the surgeon’s broad shoulders.
“No hidden drawers in here, nosy. There is a loose panel on the wall behind the bookshelf, if you haven’t checked that yet. Nothing interesting in it, but by all means, help yourself. Might as well try my office while you’re at it - there are much better hiding places in there.”
7 notes
·
View notes
Text
Modular ICU: The Future of Intensive Care Infrastructure
In today’s fast-evolving healthcare landscape, especially post-pandemic, hospitals are under constant pressure to upgrade their critical care infrastructure. One innovation leading this transformation is the Modular ICU. These advanced, prefabricated units are quickly redefining how intensive care is delivered in India.
But what exactly is a modular ICU? Why are more hospitals choosing this model over conventional ICU rooms? Let’s break it down.
What is a Modular ICU?
A Modular ICU is a pre-engineered, prefabricated intensive care unit built using cleanroom-grade components. These units use PUF-insulated panels, flush doors, aluminium coving, HEPA filters, and antimicrobial flooring to create a sterile and precisely controlled environment.
In simple terms, the modular ICU meaning refers to a compact, scalable setup designed to meet NABH, WHO, GMP, and USFDA standards. They're faster to build, easier to maintain, and provide top-notch infection control.
Why Modular ICUs Are Gaining Ground in India
There are several reasons modular ICU rooms are becoming mainstream:
Urban growth and rising patient load require hospitals to expand quickly.
Post-COVID readiness is pushing healthcare facilities to upgrade for future emergencies.
Cost efficiency matters, and modular builds reduce time, labor, and material waste.
Compliance is simpler as modular ICUs are designed with standards in mind from the start.
Scalability allows easy expansion, relocation, or modification during pandemics.
Key Features of Modular ICU Design
A modern modular ICU unit includes the following advanced components:
The walls and partitions are made of PUF insulated panels, available in 50mm to 100mm thickness, offering excellent thermal insulation and a smooth, clean finish. These panels are generally made with pre-coated GI or stainless steel.
Ceilings can be either walkable or non-walkable. They support HVAC ducts, cable trays, medical gas lines, and lighting systems while keeping contaminants out.
Flush doors made of powder-coated GI or stainless steel come with vision panels and interlocks. These doors are often hermetically sealed to maintain pressure zones and prevent contamination.
HEPA filtration systems, often combined with Laminar Air Flow (LAF) units, ensure Class 100 air purity. These systems remove particles down to 0.3 microns, offering near-sterile air quality.
Hospitals can also integrate Smart Surgeon Control Panels—touch-enabled units that manage temperature, lighting, AHU operation, and more from a single point.
Flooring is another crucial element. Options include epoxy flooring for chemical resistance and seamless design, vinyl flooring for waterproofing and cushioning, and PU flooring for anti-skid safety.
Advantages of Modular ICU Units
Here are the benefits that modular ICUs deliver:
They are 30–40% faster to install than traditional ICU builds. The surfaces are seamless and hygienic, preventing microbial growth. Due to insulated construction, energy use is reduced, helping hospitals save on HVAC costs. The units are regulatory-compliant and customizable for future expansion, whether in public hospitals or temporary setups.
Modular ICU vs Conventional ICU: What's Better?
Modular ICUs are much quicker to build—typically within 3 to 5 weeks—whereas conventional ICUs may take several months. While modular units come pre-compliant with NABH and international standards, conventional ICUs may need later upgrades.
In terms of expansion, modular ICUs are more flexible, making them ideal during pandemic situations. They also prove to be more cost-efficient in the long run, saving hospitals up to 20% on construction and operational costs.
Most-Searched Questions Answered
What is the meaning of a modular ICU? A modular ICU is a prefabricated, highly sterile intensive care environment designed for fast deployment and superior infection control.
How long does it take to build a modular ICU room? On average, it takes about 3 to 5 weeks, depending on size and complexity.
Are modular ICUs better than conventional ICUs? Yes. They are quicker, more hygienic, easier to maintain, and cost-effective.
What are modular ICU units made of? They are built using PUF-insulated panels, cleanroom-grade flooring, flush doors, HEPA filters, and advanced HVAC systems.
Are modular ICUs NABH compliant? Yes, most modular ICUs are built to comply with NABH, WHO, GMP, and USFDA standards.
Where Modular ICUs Are Used
Across India, modular ICU rooms are being implemented in public hospitals, private multispecialty centres, teaching hospitals, disaster relief camps, and even military healthcare units. Their flexibility and speed make them ideal for permanent setups and emergency expansions alike.
Best Practices for Modular ICU Installation
To ensure a successful setup:
Choose an experienced turnkey provider with in-house manufacturing.
Collaborate with architects and MEP consultants early in the design stage.
Follow ASHRAE 170 and NABH norms strictly.
Prioritize HVAC layout, pressure zoning, and airflow integrity.
Always use fire-rated, anti-microbial, medical-grade materials.
Ready to Upgrade Your ICU?
If you are planning a new hospital wing, expanding capacity, or bidding on healthcare tenders, now is the time to adopt modular ICU infrastructure. It’s cleaner, safer, and built for tomorrow’s healthcare needs.
Final Thoughts
Healthcare infrastructure is no longer about just building walls—it’s about creating safe, hygienic, and high-performance environments. Modular ICU units represent a revolutionary step forward in intensive care.
If you’re looking for a trusted partner to deliver these solutions from design to commissioning, AUM Industries brings the expertise, manufacturing capabilities, and compliance assurance you need. From modular OTs to cleanrooms and ICUs, they are a one-stop turnkey solution provider trusted by healthcare professionals across India.
📧 Email: [email protected] 🌐 Website: www.aumindustriesmfg.com

#ModularICU#ModularICURoom#ModularICUDesign#ModularICUMeaning#ModularICUUnits#HealthcareInfrastructure#HospitalConstruction#ModularHealthcare#TurnkeyHealthcareSolutions#MedicalInfrastructure#CriticalCareInfrastructure#ModularOT#CleanroomTechnology#CleanroomSolutions#HEPAFiltration#HVACDesign#NABHCompliance#GMPCompliance#USFDAStandards#HealthcareInnovation#HospitalDesign#ICUDesign#MedicalTechnology#SmartHospitals#FutureOfHealthcare#MakeInIndia#HealthcareIndia#HospitalProjectsIndia#ModularICUIndia#TurnkeySolutionsIndia
0 notes
Text
Choosing the Right IVF Doctor in Bangalore: 620 Words to Guide Your Parenthood Journey
Bangalore—India’s vibrant technology hub—has also emerged as a powerhouse for fertility care. Couples and individuals from every corner of the country, and increasingly from abroad, travel here seeking world-class reproductive medicine delivered at sensible prices. Yet the abundance of clinics can feel overwhelming when you’re trying to pick the perfect ivf hospital in bangalore. This guide breaks down the qualifications, technologies, and patient-centric qualities that distinguish top specialists, and offers practical tips to help you begin treatment with confidence and clarity.

1. Why Bangalore Leads India’s Fertility Landscape
Cutting-edge laboratories. Most leading centers are equipped with time-lapse embryo culture, AI-based grading, pre-implantation genetic testing (PGT-A/PGT-M), laser-assisted hatching, and vitrification. Such innovations rival Western programs while typically costing 40 – 60 % less.
Globally trained clinicians. Many doctors hold fellowships from ESHRE or ASRM, ensuring they apply international protocols to Indian contexts. Their expertise directly translates into higher live-birth rates, particularly for complex female-factor and recurrent implantation failure cases.
Comprehensive, one-roof care. The city’s best clinics integrate reproductive endocrinologists, laparoscopic surgeons, embryologists, andrologists, geneticists, dietitians, and counselors. This synergy minimizes referrals and streamlines the patient journey.
2. Credentials That Matter
Formal sub-specialization. Seek an MD or DNB in Obstetrics & Gynaecology followed by an FNB, FRM, or MCh in Reproductive Medicine. A decade of ART-specific experience is ideal.
Laboratory accreditation. NABH, CAP, or ISO 15189 certification confirms rigorous quality control—vital for safeguarding gametes and embryos.
Transparent outcome data. Reputable doctors publish age-stratified live-birth rates, not just “positive test” numbers. Always ask to see independent audit figures.
Continuing education. Membership in professional bodies (e.g., Indian Fertility Society, ISAR) and frequent conference presentations signal a commitment to staying current.
3. Diagnostic Cornerstones
Extended hormone profiling. Beyond day-2 FSH and LH, top specialists assess AMH, prolactin, thyroid markers, and DHEA-S to tailor stimulation plans.
High-resolution imaging. 3-D saline infusion sonography and Doppler studies reveal subtle uterine anomalies or blood-flow issues that could hamper implantation.
Male-factor deep dive. Computer-assisted semen analysis, DNA fragmentation assays, and scrotal Doppler scans uncover causes often missed in routine checks.
4. Treatment Innovations Boosting Success
Challenge
Game-Changing Solution
Typical Benefit
Low ovarian reserve
Duo-stim (double stimulation) in one menstrual cycle
Up to 20 % rise in oocyte yield
PCOS anovulation
Letrozole induction plus myo-inositol + vitamin D
15 % higher ovulation rate
Severe male factor
Micro-TESE combined with ICSI
Viable sperm retrieved in 45 – 60 % of non-obstructive azoospermia cases
Recurrent miscarriage
PGT-A and immunological work-ups
Miscarriage risk cut by ~50 %
5. Hallmarks of Patient-Centric Care
Lifestyle integration. Leading doctors pair medical protocols with Mediterranean-style nutrition plans, individualized exercise regimens, and supplements proven to enhance gamete quality.
Mental-health focus. Certified counselors, CBT sessions, and mindfulness workshops lower treatment stress—research shows stress reduction may improve implantation rates.
Flexible protocols. Mild-stimulation IVF, freeze-all strategies, and personalized embryo-transfer timing accommodate diverse ovarian responses and endometrial receptivity profiles.
6. Practical Steps Before Your Consultation
Collect prior records. Hormone panels, ultrasound images, laparoscopy notes, semen analyses, and past stimulation sheets prevent redundant testing.
Prepare financial questions. Clarify whether quotes include medications, ICSI, PGT, anesthesia, freezing, and follow-up consults. Hidden fees cause needless anxiety.
Plan logistics. A standard antagonist protocol requires daily scans for about 10 – 12 days; consider serviced apartments in Indiranagar, Koramangala, or Jayanagar for easy clinic access.
7. Community Support & Post-Treatment Care
Top Bangalore clinics host monthly peer forums where graduates share real-life stories of overcoming endometriosis, repeat failures, or donor-egg journeys. These gatherings provide invaluable insights—from injection hacks to coping with the “two-week wait.”
8. Taking the First Step
Shortlist two or three ISO-accredited ivf doctor in bangalore centers and schedule complementary video calls. Gauge how clearly the doctor explains protocols, success metrics, and backup plans. The best infertility specialist in bangalore will combine technical mastery with empathy, empowering you to make informed decisions every step of the way.
0 notes
Text
CoolSculpting: Freeze Away Fat Without Going Under the Knife
The landscape of plastic surgery in London has shifted dramatically with the rise of non-invasive procedures, and CoolSculpting has emerged as one of the most sought-after treatments for body contouring without surgery. By freezing stubborn fat cells, this revolutionary method provides a slimmer, more sculpted figure—without needles, anaesthesia, or downtime.
CoolSculpting in London has been gaining attention for its ability to target areas of fat that are resistant to diet and exercise. Common treatment areas include the abdomen, thighs, flanks, back, and under the chin. With visible results and no recovery time, it is considered a game-changer in the world of aesthetic medicine.
Why a London Plastic Surgeon Should Be Chosen for CoolSculpting
Although CoolSculpting is a non-surgical procedure, it is often advised that treatment be carried out by a qualified London plastic surgeon. When handled by an expert, the sculpting process is safer, more precise, and tailored to suit the individual’s goals and body type.
The procedure works by applying controlled cooling to fat cells beneath the skin, a process known as cryolipolysis. These fat cells are frozen and gradually eliminated by the body over several weeks. Unlike weight loss, which shrinks fat cells, CoolSculpting reduces the number of fat cells in the treated area, offering long-term results.
Body contouring in London has evolved thanks to CoolSculpting, which has been widely adopted in reputable cosmetic practices and clinics across the city.
Trusted by Leading Cosmetic Surgeon London Experts
A cosmetic surgeon London patients trust will perform a full consultation before treatment to determine eligibility and design a customised plan. The targeted areas are mapped out, and cooling panels are placed on the skin to freeze the fat safely and evenly.
During the session, patients typically feel a cold sensation followed by numbness. The process is comfortable enough that reading or relaxing during the treatment is common. Each session lasts about 30 to 60 minutes, depending on the area treated.
Multiple sessions may be recommended to achieve optimal results, especially for those looking to treat more than one area or reduce a higher volume of fat.
CoolSculpting in London has proven to be effective for individuals with a stable weight who are looking to refine and shape their physique rather than dramatically lose weight. It is not a substitute for diet or exercise, but it works exceptionally well as a targeted fat-reduction tool.
How Plastic Surgery in London Has Expanded with Non-Surgical Solutions
For many years, plastic surgery in London was associated mainly with procedures that required incisions and recovery periods. CoolSculpting has redefined the industry by offering a non-invasive solution that produces impressive results with little to no disruption to daily life.
Fat freezing in London is now commonly requested by those who want to address areas of fat that haven’t responded to lifestyle changes. Because there are no cuts or anaesthesia involved, the risks associated with surgery are avoided.
In the weeks following treatment, the frozen fat cells break down and are naturally flushed out by the body. Improvements begin to appear after three weeks, with full results seen within two to three months.
Why a Cosmetic Surgeon London Based is Best for Fat-Freezing Treatments
Choosing a cosmetic surgeon London based for CoolSculpting ensures that the highest standards of care and safety are maintained. Professional oversight allows for accurate assessment, effective fat mapping, and results that align with natural body contours.
Patients are also guided through post-treatment care, including tips on maintaining results through a balanced lifestyle. While the fat cells removed through CoolSculpting do not return, maintaining a stable weight is recommended to preserve the outcome.
CoolSculpting in London is also frequently combined with other non-invasive treatments for even more refined results, such as skin tightening or cellulite reduction.
CoolSculpting has made it possible to contour the body and reduce fat without going under the knife. With the guidance of a London plastic surgeon, the procedure delivers noticeable, natural-looking results without the recovery period of traditional surgery.
For anyone exploring plastic surgery in London but hesitant about surgical options, fat freezing offers a safe and effective alternative. Trusted cosmetic surgeon London clinics continue to lead the way in offering this treatment, helping individuals achieve a more sculpted appearance—quickly, comfortably, and confidently.
0 notes
Text
Ot light manufacturers in delhi
OT Light Manufacturers in Delhi: Illuminating the Future of Surgery In the ever-evolving healthcare industry, precision and clarity are critical, especially in operation theatres where lives are saved every day. One of the most essential elements in any surgical setup is the OT light — a surgical lighting system designed to provide bright, shadow-free, and focused illumination during operations. In recent years, OT light manufacturers in Delhi have played a vital role in developing world-class solutions that meet international standards at competitive prices.
Let’s explore why Delhi has become a hub for OT light manufacturing, what to look for in a quality OT light, and the top features that modern medical institutions seek in these critical devices.
What Are OT Lights? OT lights, short for Operation Theatre lights, are medical-grade lighting systems used during surgeries and medical examinations. These lights help doctors and surgeons perform procedures with utmost accuracy by offering:
Consistent brightness
Adjustable focus
Shadow-free illumination
Cool, white light to reduce heat emission
OT lights are available in various types such as LED surgical lights, ceiling-mounted lights, mobile OT lights, and wall-mounted variants, depending on the operating room’s design and the nature of surgeries.
Why Delhi is a Key Market for OT Light Manufacturing Delhi is not just India’s capital; it is also a growing medical equipment manufacturing hub. Here are a few reasons why many hospitals and distributors rely on OT light manufacturers in Delhi:
Established Manufacturing Ecosystem Delhi NCR (including Noida, Ghaziabad, and Faridabad) houses several ISO-certified medical device manufacturers that supply across India and export globally.
Proximity to Government and Private Hospitals With numerous hospitals, medical colleges, and government tenders based in or around Delhi, manufacturers find it easier to serve their clients directly.
Cost-Effective, High-Quality Solutions Delhi-based companies often provide international-quality OT lights at far more competitive rates compared to imported brands, making them a preferred choice for budget-conscious institutions.
Customization and After-Sales Support Manufacturers here offer personalized solutions based on surgical specialties like cardiology, neurosurgery, and orthopedics — along with responsive technical support.
Types of OT Lights Manufactured in Delhi Delhi-based OT light manufacturers offer a broad product range to cater to different hospital setups:
LED OT Lights Energy-efficient, long-lasting, and cooler than halogen lights. Ideal for modern modular OTs.
Ceiling-Mounted OT Lights Perfect for fixed installations in operation theatres, offering a clear, overhead view with minimal obstruction.
Mobile OT Lights Flexible and portable, used in smaller clinics, emergency rooms, or as backup lighting systems.
Single Dome & Double Dome Lights Single dome lights are suited for general surgeries, while double dome lights provide wider illumination for complex procedures.
Shadowless Lights Designed with multi-reflector technology to ensure minimal shadows during surgery.
Key Features to Look for in OT Lights When selecting a manufacturer or product, hospitals should prioritize the following:
High Lux Intensity (100,000+ lux)
Adjustable Color Temperature (3500K–5000K)
Heat Management System
Sterilizable Handle for Surgeons
Battery Backup for Emergency Use
Arm Rotation Flexibility
Digital Control Panel for Adjustments
Most OT light manufacturers in Delhi also ensure their products comply with IEC, CE, ISO 13485, and BIS certifications for safety and performance.
Top OT Light Manufacturers in Delhi Several well-established brands are operating from Delhi, offering reliable and innovative OT lighting systems. Some of the reputed names include:
Hospi Lights A leading name in surgical lighting and OT table manufacturing. Offers both standard and premium models for hospitals and clinics.
Technomed India Offers a wide range of ceiling and mobile OT lights with advanced LED technology. Known for exporting to multiple countries.
Desco India Manufactures and supplies operation theatre equipment, including OT lights, across government and private medical institutions.
Meditech India Known for affordable, customizable OT lighting solutions with smart features like remote control, color temperature adjustment, and zero heat technology.
Applications of Delhi-Made OT Lights Government Hospitals
Private Nursing Homes
Multi-Specialty Hospitals
Veterinary Clinics
Medical Colleges
Daycare Surgical Centers
With growing healthcare infrastructure across tier-2 and tier-3 cities, Delhi’s manufacturers are also fulfilling orders pan-India and internationally.
Final Words If you’re searching for durable, affordable, and high-performance surgical lighting systems, then choosing a reliable OT light manufacturer in Delhi is a smart move. From advanced LED lights to modular operation theatre setups, these manufacturers offer end-to-end solutions backed by quality, support, and innovation.
Before purchasing, always review the manufacturer’s experience, technical specifications, warranty terms, and service reach to make the best decision for your healthcare facility.
0 notes
Text
Immunology Hepatitis B and C virus transmission during surgical interventions has become a critical concern. Healthcare workers are especially prone to catch HBV and HBC infections from patients and vice versa. Statistics derived from several studies over the last decade and a half reveal a 4% infection rate for patients of surgeons who are positive for HbeAg. This study under consideration by Harpaz et.al (1996) analyzes this important clinical issue of transmission of the HBV from a previously infected surgeon to his patients. The Physician under study tested positive for the hepatitis B surface antigen (HBsAg) and anti-HBc (antibody) and was diagnosed with jaundice in February 1992. However, by March 1992 when he symptomatically recovered, he resumed his duties as a surgeon in two hospitals. This retrospective cohort study analyzed the period between July 1991 and July 1992 and reviewed a total of 144 patients who received surgical care from the particular doctor. The researchers used chart reviews, interviews and serologic testing for patients who received surgical care from the physician under study in two hospitals where he was working during the aforementioned study period. A total of 19 patients out of 144 (13%) study subjects (those who were operated by the surgeon) developed HBV infection post surgery. As a control group, the researchers also observed 124 patients who received surgical care from other thoracic surgeons in one of the hospitals under study. This was useful in identifying any other hospital-based potential infection sources. However, the fact that none of these 124 subjects were positive for HBV post surgery clearly ruled out infection by other nosocomial sources. Serological testing further revealed that the HBsAg subtype adW2 found in the surgeon was common in 13 infected subjects. Further HBV DNA sequence from the surgeon matched that of 9 case subjects who were also tested. Thus the study rightly identified the doctor under study to be the source of infection. The researchers reported to have identified traces of HBV DNA and HBsAg from the lesions that were formed during the one-hour suture simulation test. This retrospective study concluded that the lesions formed during suturing in combination with glove failure could have been the possible route of transmission of the HBV. However, the study failed to point out any conclusive evidence as to the route of transmission. It was revealed from the study results that cardiac transplantation procedure (relative risk, 4.9; 95% confidence interval, 1.5 to 15.5) carried greater risk factor for HBV infections. The one big drawback of this study is the vagueness of the results. Though the source of infection is clearly established, the researchers were not able to pinpoint the exact route of transmission. Furthermore, it is clear from the information that was directly gathered from the surgeon that he had clearly violated atleast one of the standard of surgical procedures. The surgeon had admitted to applying hemostatic material to sternal incisions without the use of sponges, which is not recommended due to the possibility of glove tears and percutaneous contact. Therefore, there is atleast some evidence for 'inadequate infection control'. However, it must be added that the rare percutaneous exposure does not account for the high rate of infection as identified in this study. Since it is well-known that HB infections tend to be asymptomatic in almost 70% of the cases, it increases the risk factor of the physician transmitting the virus unknowingly. Health care workers (HCW) who perform invasive procedures are obligated to know their serological status for HIV, HB and other chronic infectious conditions. Medical practice of HBeAg-positive health care worker should be carefully monitored and restricted as the health Canada panel recommended recently. Blatant or negligent violations in this respect, on the part of the surgeon, may in fact be regarded as a biocrime. The article under study and some other studies have shown that even with adherence to the recommended infection control procedures, the transmission of HBV from surgeon to patient continues to be a problem. Though the study discussed here suffers from vagueness relating to the mode of transmission, it has clearly exposed the source of the infection. The study also suggests that patients undergoing immunosuppressive therapy maybe at a greater risk for catching HBV infections. There is enough justification to limit the practice of HB infected physicians from exposure prone procedures. As the study under review concludes, HBV vaccination would have saved the doctor all the trouble that he caused inadvertently to his patients and to himself. It may not be far fetched to make HBV vaccination an essential for obtaining operating room privileges. Bibliography 1) Gerlich WH, 'Hepatitis B and C. Risk of transmission from infected health care workers to patients' Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz., 2004 Apr;47(4):369-78 2) Rafael Harpaz MD & Lorenz Von Seidlein et.al, 'TRANSMISSION OF HEPATITIS B VIRUS TO MULTIPLE PATIENTS FROM A SURGEON WITHOUT EVIDENCE OF INADEQUATE INFECTION CONTROL', NEJM, 1996, Vol 334, no 9. 3) American College of Surgeons, 'Statement on the surgeon and hepatitis', Bulletin of the American College of Surgeons, Vol.89, No. 4, April 2004 Available From, http://www.facs.org/fellows_info/statements/st-22.html 4) Shirley Paton, RN, MN; Shimian Zou, MD, PhD; Antonio Giulivi, MD, FRCPC, 'More Should Be Done to Protect Surgical Patients From Intraoperative Hepatitis B Infection', Infection Control and Hospital Epidemiology, Vol. 23 No. 6, 303- 305, Available From, http://www.journals.uchicago.edu/doi/pdf/10.1086/502055?cookieSet=1 5) Spijkerman IJB, van Doorn L-J, Janssen MHW, et al. Transmission of hepatitis B virus from a surgeon to his patients during high-risk and low risk surgical procedures during 4 years. Infect Control Hosp Epidemiol 2002;23:306-312. Read the full article
0 notes
Text
Daredevil (vol. 1) #147: Breaking Point!
Read Date: November 11, 2023 Cover Date: July 1977 ● Writer: Jim Shooter ● Penciler: Gil Kane ● Inker: Klaus Janson ● Colorist: Klaus Janson ● Letterer: Denise Wohl ● Editor: Archie Goodwin ●

**HERE BE SPOILERS: Skip ahead to the fan art/podcast to avoid spoilers
Reactions As I Read: ● uh-oh, he gonna be glomped to death ● police surgeon? is there such a thing? ● David Tennant made me adore Kilgrave (I know it’s Killgrave, but I prefer the Netflix spelling)

● they dragged on Debbie’s kidnapping for months… then just resolve it within a few panels? ● though I’m not wholly in love with the art, I do appreciate that DD isn’t quite so jacked ● 👏👏👏
Synopsis: Exiting the studio where he defeated Bullseye on live TV, Daredevil is swarmed by an admiring crowd. They press in on him until he leaps up to the rooftops to collect himself. That night, with the clue provided by Bullseye he bursts into the offices of Maxwell Glenn, who with minimal prodding confesses to several crimes, including the kidnapping of Debbie Harris. DD forces his to confess to the police as well, but before they can arrive, the Purple Man reveals himself as pulling Glenn’s strings all along.
Elsewhere, Debbie Harris pleads with her kidnapper to let her go, to no avail. But then Daredevil bursts in and rescues her. Later, speaking with Debbie and Foggy, Heather Glenn witnesses her father being arrested. He says he doesn’t remember anything about his crimes. Matt senses that Heather wishes Matt were around, but DD cannot appear as Matt Murdock until his shoulder heals.
Beginning to suspect there is more to the story, DD returns to Maxwell Glenn’s office, and discovers a secret door, behind which the Purple Man is pontificating about the criminal empire he has been building behind the scenes. Killgrave acknowledges that DD has resisted his powers in the past, but says he has since grown stronger. He exerts his will on DD, but still cannot take control of him. Instead he orders the other businessmen to attack him, but an enraged DD knocks out the lights and defeats them all, vowing he will end Killgrave.
One of the stooges gets a lucky shot on his damaged shoulder, delaying DD just long enough for Killgrave to escape.
(https://marvel.fandom.com/wiki/Daredevil_Vol_1_147)

Fan Art: Daredevil by WeijiC
Accompanying Podcast: ● Josh and Jamie Do Daredevil - episode 26
#marvel#marvel comics#my marvel read#podcast recommendation#podcast - josh and jamie do daredevil#comics#comic books#daredevil#matt murdock#fan art#fanart
1 note
·
View note
Text
Enhancing Surgical Robot Navigation with Mobile 3D Flat Panel C-arm Imaging
In recent years, surgical robotics has been widely used and robot-assisted surgery has become increasingly popular worldwide.

What Is a Mobile 3D Flat Panel C-arm?
Unlike conventional spiral CT used in radiology departments, mobile 3D flat panel C-arms utilize cone-beam CT technology. This compact, maneuverable system can be easily deployed in operating rooms and provides high-resolution, 3D intraoperative imaging. Devices such as the Perlove Medical PLX C7600 exemplify this technology, particularly in spinal and orthopedic procedures.
Let’s explore how mobile 3D C-arm systems assist surgical robots in four key steps during spinal surgery:
1. Intraoperative Image Acquisition
In orthopedic procedures—especially spinal surgeries—real-time visualization of bone structures is essential. Compared to MRI, intraoperative C-arm imaging is often the preferred solution due to its superior ability to render bone anatomy with high accuracy.
Mobile 3D flat panel C-arms allow the acquisition of multiple fluoroscopic images during surgery. These are sent to a workstation where a 3D reconstruction is generated, offering real-time updates of the patient’s anatomy. The most advanced systems even support automatic 3D reconstruction using preoperative data, ensuring that what surgeons see during the procedure truly reflects the current anatomical conditions.
2. Motion Capture for Real-Time Tracking
Accurate surgical navigation depends heavily on motion capture systems that track the spatial positioning of surgical instruments. In spinal surgery, optical tracking is most commonly used.
These systems use cameras to triangulate the exact position of surgical tools in three-dimensional space. To maintain tracking accuracy, the surgical team must ensure an unobstructed line of sight between the cameras and instruments throughout the procedure.
By integrating with the surgical robot, motion capture allows the system to track tool movement and orientation in real time—providing a live view of surgical instrument trajectories with sub-millimeter accuracy.
3. Image Registration for Surgical Precision
Image registration is the process of aligning intraoperative images with the patient’s actual anatomy, effectively creating a navigational “map” for the robotic system.
For example, Perlove Medical’s Spine Surgical Navigation System PL300B automatically performs this step by tracking the movement of the C-arm during 3D image acquisition. This method, known as trajectory-based registration, offers several advantages:
Not reliant on image quality
Higher registration precision
Fewer manual steps
Improved system efficiency

4. Real-Time Image Visualization
Once registration is complete, the navigation system overlays a virtual representation of the surgical instrument onto the 3D images captured by the C-arm. As the surgeon maneuvers the tool, its digital counterpart moves accordingly on the screen.
This real-time visualization allows the surgeon to evaluate the spatial relationship between the instrument and the patient’s anatomy continuously. The result is more accurate targeting, enhanced control, and a higher degree of confidence during delicate tasks like pedicle screw placement in spinal surgery.
The Impact: Safer, Smarter, and Faster Surgery
The integration of mobile 3D flat panel C-arm imaging with surgical robotic systems delivers transformative benefits:
Higher accuracy in screw placement
Lower complication rates
Reduced radiation exposure for staff and patients
Minimized bleeding and postoperative pain
Shorter recovery times and hospital stays
By combining advanced imaging and robotics, this approach not only enhances clinical outcomes but also improves the overall surgical experience for both patients and healthcare providers.
0 notes
Text
[ID: Ten panels of text, some in boxes and word bubbles, against different colored sort-of marbled textured backgrounds.
Panel 1 :
Eventually there were no more surprises.
Just grimly hanging on for the rest of the infusions
Five more. Four more... Three more... Two more... One more...
Done
I didn't really believe it was over, though.
It didn't seem possible.
Panel 2 :
Five months is a long time to do anything
When the next week rolled around and I didn't have chemo, it felt strange.
I was also exhausted
"Ok, yeah, I see what they mean by "cumulative." Zzz..."
All the news was great. I had scans and another MRI and they showed that Tumor-Bob had shrunk by 98%. It had all been a rousing success.
I should have felt happier about that.
Panel 3 :
Don't get me wrong, I wasn't unhappy about it
I just kept waiting for the relief. You know, the great weight lifting.
"Any minute now..."
But it didn't happen
It didn't feel like it was almost over. It didn't feel like a thing that could be over.
Panel 4 :
"Maybe after surgery," I thought
Surgery was scary. I had total faith in my surgeon, but this was still uncharted territory.
Was I gonna have a weird boob divot?
Was I gonna have edema from the lymph nodes being removed?
Was I gonna die on the table from the anesthesia and a previously unknown allergy?
I'd hated chemo but at least I knew the next thing to expect
Spoiler Alert: I did Not die on the table
I woke up with a massive incision in my armpit and an ugly scar across the side of my boob. Oddly, I wasn't that upset.
If you're gonna have cancer, might as well get an impressive-looking scar.
Panel 5 :
There was a slight disagreement about painkillers
Dr. : "Lots of patients get by just on tylenol!"
"Give me oxycontin or give me death."
Dr. : "Um---"
"I am Not selling these on the black market. If the black market tries to take them, I will beat it to death with a chair."
They gave me more painkillers
My breast didn't hurt at all. It was my armpit that was killing me. Armpits are like knees - they connect to everything and you don't notice until they go bad.
Also I had to wear a sports bra day and night for two weeks.
Panel 6 :
The surgeon called the next day
They got it all. I didn't have cancer any more.
Huh.
My Mom and my Husband and about a thousand people on the internet were Ecstatic.
It was weird. I think I felt happier that they were happy than anything else. It didn't seem terribly real to me.
In the past, I’ve won major awards, and I never quite believed it at the time. It wouldn't be until like six months later that it would sink in. Of course, by then everybody's moved on and it feels weird to talk about it.
This was Not an award.
"This better not be one of those Delayed-Action PTSD things..."
Panel 7 :
But then I started to feel worse
And worse... and worse...
Pretty soon I was close to bedridden. When I stood up, my legs hurt a lot. I was exhausted. Also I stopped eating almost completely, which it turns out isn't good for your energy levels either.
"Is this from the chemo?"
It wasn't.
"Is it the drugs?"
It wasn't
"Long COVID?"
It wasn't
[In a broken-line word bubbble, like a whisper] "Is it gonna be like this forever...?"
Panel 8 :
At that point, my oncologist stepped in.
Dr. : "I do not know what is wrong, but I Will find out."
"Oh thank god"
And she did.
It turned out that one of the immunotherapy drugs I had taken months earlier taught my immune system to attack cancer cells. (Amazing stuff, really.)
Unfortunately, in less than one percent of patients, it taught the immune system to attack other cells too.
My pituitary gland was now dead in the water.
The pituitary tells the adrenal glands to make cortisol
Panel 9 :
You hear about the bad effects of high cortisol levels, but let me tell you, having none at all is Much Worse.
Cortisol is one of those chemicals that control about fifty different things. I would have eventually gone into Shock and ended up in the ICU with Acute Adrenal Failure.
My doctor figured it out and had me on replacement cortisol in two days.
Fortunately, it's an easy fix. I would probably be getting my cortisol in pill form for the rest of my life, and I had to get a MedicAlert bracelet, but that was all.
"Eh, still better than cancer."
I felt better so fast that it was almost ridiculous
After that interlude, Radiation was practically a non-event. I drove to the clinic five times a week for a month, got a hellacious sunburn on my underboob, and then was done.
Panel 10 :
And that was it.
I got my port out. It was an incredible piece of technology and I hated it So Goddamn Much.
I had some follow-up appointments. Everyone agreed I was fine. There was a chance Bob might come back, but not a big chance.
It's been a few months now. My hair is growing back in. I'm slower and I need to rest a little more often, but not that much more often.
I visited Australia for the first time and spent five hours wandering around the Melbourne Botanical Gardens after birds. I did a pretty intense book tour. And... I was okay.
It's starting to feel like cancer is a thing that happened, not something that will always be happening.
I wish I had something clever or meaningful or uplifting to say, but I don't. Maybe there doesn't always have to be a moral. You don't have to come out a better and wiser person. Sometimes random shit just happens and it sucks and you go on.
See you in hell, Bob.
"Good riddance!"
/end ID]
The Saga of Bob: Endgame (hopefully)
This one was awhile coming. Partly I was afraid that if I posted it, the tumor would come back the next day, and partly I had some complications that took awhile to iron out. But here we are, at long last, sans Bob.
You can learn all about how I had cancer in Part One or hit the prior episode at Part Seven.
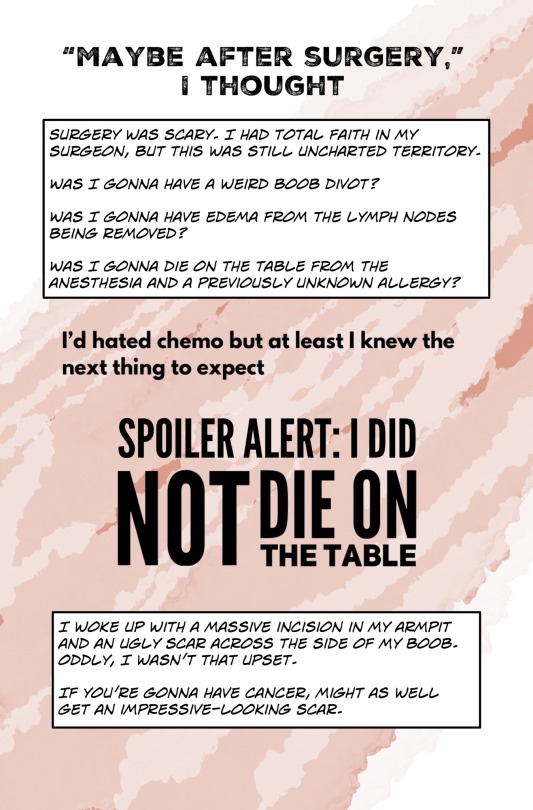
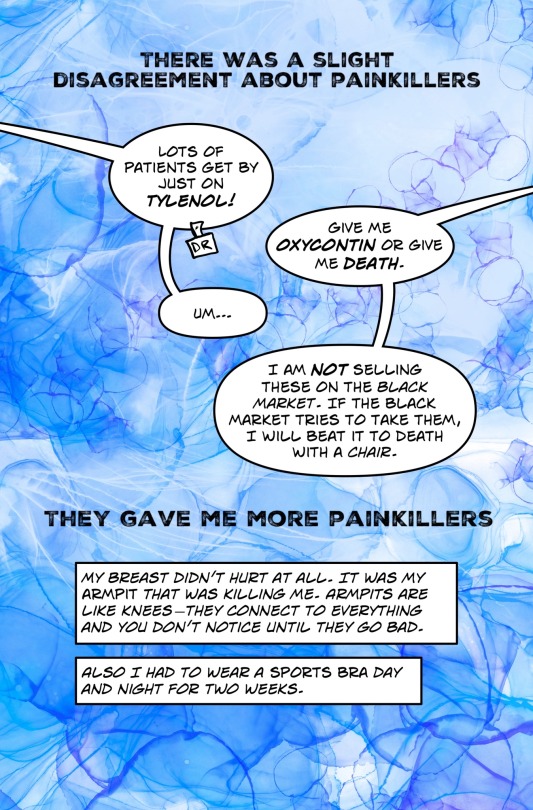
What is with doctors and painkillers?! Though to her credit, she was like “I am so sorry you’re in pain! Let me write a new prescription!”
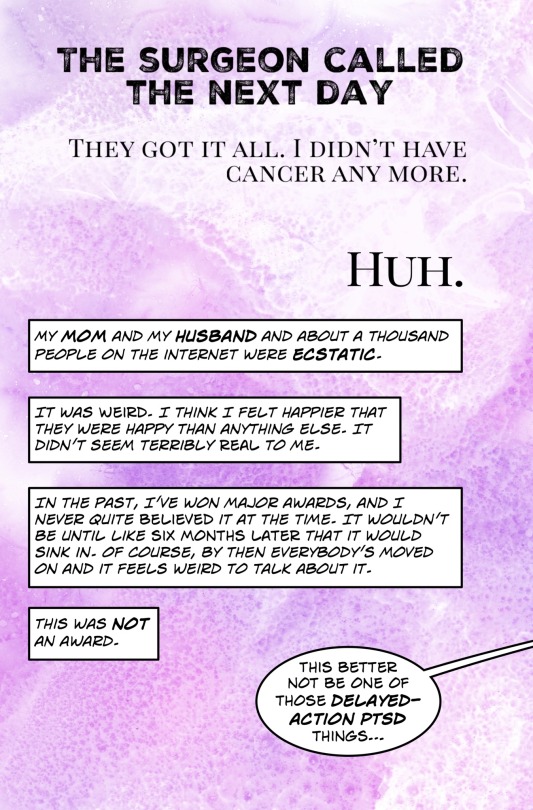
(Still not sure if it’s PTSD.)
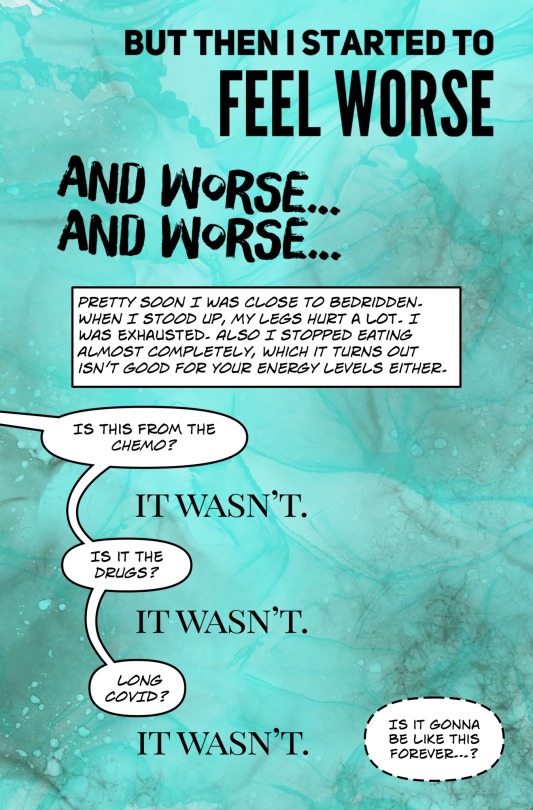
That last bit was the really scary one. (It was, uh, pretty bad. Never been bedridden before. Don’t recommend it.)
Shout out to Doctor Pinkeye who had it sorted in two business days. Also, when I first reported my symptoms, she said “You never complain about anything. If you say something’s wrong, it is.” She’s a doctor in a million.

Lack of cortisol can cause problems in about twenty different ways, including dangerous levels of potassium and blowing your electrolytes all to hell. It’s actually kinda interesting, in a “wow, look at all the fascinating ways I could keel over!” way.
Honestly, after two months of slowly crashing cortisol levels, complaining about radiation would have felt like complaining over a hangnail. It was boring and I moisturized a lot, the end.
Also there are some quite nice MedicAlert bracelets on Etsy.
And here is hoping I never have to make another one of these!
2K notes
·
View notes